The term medical-grade is frequently used as a marketing label to justify high prices for mobile hardware. However, in a hospital ward at 3:00 AM, a device is only as good as its ability to survive “survival use.” This case study explores the development of a medical handheld PDA, moving past brochure specifications to address the chemical, mechanical, and human friction that defines clinical success.
Also Read: Rugged Tablet Casestudy
1. Project Overview
We partnered with a healthcare integrator to develop a mobile solution for hospital IT system providers. The goal was to replace fragmented, consumer-grade hardware with a single, reliable Android platform designed for the high-intensity hospital workflow.
Application Scenarios
The device was engineered to serve four critical pillars of hospital operations:
- BCMA: Verifying patient identity and dosage at the bedside.
- Electronic Medical Record: Providing real-time data entry and retrieval for doctors and nurses.
- Specimen Tracking: Ensuring lab samples are labeled and tracked without manual entry errors.
- Inventory Management: Managing high-value surgical assets and medication stocks across multiple departments.
Project Objective
The client needed a device that could keep working through nonstop hospital use, day and night, for around 5 to 7 years. Because of that, the hardware had to be made for tough conditions. It needed to handle daily sterilization, keep wireless performance stable even in lead-shielded areas, and also protect sensitive patient data in line with HIPAA requirements.
2. Client Requirements and the IP Rating Trap
During the initial phase, the technical requirements focused heavily on IP ratings. However, my experience shows that a high IP rating is often a distraction in a hospital setting.
2.1 The Counter-Intuitive Truth about IP Ratings
An IP67 rating indicates a device survives a dunk in a water tank under lab conditions. It does not tell you if the device survives 5,000 wipes with Sani-Cloth or 70% Isopropyl Alcohol. In practice, chemical resistance and reprocessing validation are more important than a “waterproof” badge.
Many teams read IEC, which is for home healthcare devices, and think it also proves the device is strong enough for hospital use. This is not right. It is a different case. For equipment used in hospitals, the device must comply with IEC for general safety and IEC for EMC immunity. These standards are important because they check whether the device can still work properly when there is electrical disturbance around it. So the issue is not only about the body being sealed or protected from dust.
2.2 Functional and Safety Requirements: Made for the Hospital Ward
A hospital ward is a hard place for electronic devices. The lights are strong. Staff use gloves all the time. There is also always a risk of contamination. Because of this, the hardware cannot be weak. It has to survive daily hospital work without causing problems.
Touchscreen that works with gloves
Most normal capacitive touchscreens do not work well with gloves. If there is moisture, the problem becomes worse. To deal with this, we used a 5.5-inch high-sensitivity touch panel with a special controller. It can detect touch through latex gloves, nitrile gloves, and even double surgical gloves. This is useful in real work. A nurse should not need to remove gloves only to sign for a medicine. That wastes time and creates unnecessary hassle.
Wi-Fi 6 for busy hospital areas
Inside a hospital, a weak connection is not a small issue. It can become a safety problem. For this reason, we used dual-band Wi-Fi 6. Wi-Fi 6 performs better in crowded areas than older Wi-Fi standards. In places like nursing stations, many devices try to connect at the same time. When that happens, Wi-Fi 6 helps the Electronic Medical Record system keep running without delay or timeout.
Display made for long night duty
Night shifts are very tiring, especially for the eyes. Because of that, we added Low Blue Light display technology. This is not just a software setting. It is built into the hardware itself. It lowers the amount of high-energy blue light coming from the screen. This helps reduce eye strain. It may also help staff who work 12-hour night shifts by causing less disturbance to their normal body rhythm.
2.3 Data Security and Privacy
Patient privacy is not optional. A single lost device can lead to a massive HIPAA violation and heavy fines. We built the security into the “foundational” layers of the hardware, not just the software.
Hardware-Backed Secure Boot
Each time the device starts, it first checks if the system is genuine. A secure digital check takes place between the operating system and the key already stored inside the SoC by the manufacturer. If the signature does not match, or if the system finds any unapproved change such as rooting, the device does not continue booting. It stops there. This helps prevent malware from entering deep into the system and capturing patient data at the kernel level.
AES-256 Encryption at Rest
We implemented AES-256 hardware encryption for all internal storage. This is the industry gold standard. Even if someone physically removes the flash storage chip, the data remains a scrambled, unreadable mess without the unique hardware key buried inside the processor’s “vault.”
Full MDM Compatibility
Hospital IT departments must have total control. Our device supports a wide range of MDM solutions. This allows IT to:
- Push “Zero-Touch” updates to the entire fleet.
- Lock the device into a specific app (Kiosk Mode).
- Remote Wipe: If a device goes missing, IT can instantly delete all patient data remotely, ensuring the hospital stays compliant and protected.
3. System Architecture and Platform Selection
If an SOC is stopped too early, the manufacturer may be forced to redesign the whole product. That also brings expensive software re-validation and fresh regulatory submissions. To avoid this problem, we did not go with consumer-grade chipsets. Instead, we selected industrial Qualcomm Snapdragon silicon made for longer market availability.
3. System Architecture
In a hospital, hardware stability is the priority. If an IT director manages a fleet of 500 devices, they require a single, consistent software image. We chose a platform that remains in the supply chain long enough to prevent “hardware fragmentation” across the facility.
3.1 SoC Platform Selection: The Industrial Reality
Our chipset selection followed three strict requirements. If the silicon failed one, it was rejected.
Seven-Year Availability
We secured a guarantee that this specific SoC would remain available for seven years. This prevents the “forced upgrade” cycle seen in consumer electronics. It allows hospital systems to standardize their Android configurations and security certificates for the long term.
Thermal Management
Medical devices are often used in protective cases for 12-hour shifts, leaving no room for heat dissipation. If a chip runs hot, it throttles performance. This causes the scanner interface to lag, creating clinical friction. We selected a chip with a low Thermal Design Power (TDP) to ensure the device stays below skin-temperature comfort levels during heavy use.
Hardware-Backed Security
The chip also has a Trusted Execution Environment, or TEE. You can think of it like a secure hardware vault. It stores encryption keys in a protected area, which helps the device stay ready for HIPAA related security needs. Moreover, it supports Android Enterprise Recommended standards. Because of this, soc is able to receive security patches for up to five years.
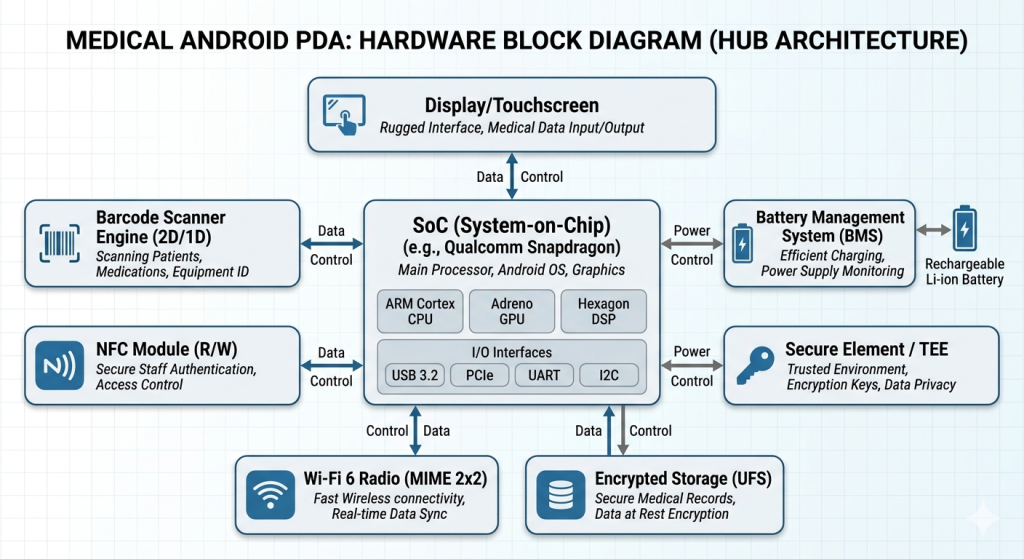
3.2 High-Density Hardware Architecture
The internal layout was engineered to remove data bottlenecks. In a high-stress ward, a half-second delay feels like a system failure.
Dedicated Scanner Bus
Many generic PDAs route scanner data through a slow internal USB-to-serial bridge. We utilized a dedicated high-speed parallel bus for the SE4710 imager. The result is zero-latency data capture. The barcode populates the EMR field the instant the trigger is pulled.
NFC Antenna Placement
We positioned the NFC antenna at the top-rear, away from the battery’s metal shielding. We tuned the signal gain specifically for nurses wearing nitrile or latex gloves. This ensures “Tap-and-Go” authentication works on the first try without the user hunting for a connection point.
Advanced Battery Management (BMS)
Charging a device 24/7 in multi-slot docks is physically brutal on lithium cells. Our BMS uses Texas Instruments gas-gauging technology to monitor cell chemistry. If the device is too hot from a long shift, the BMS slows the charge rate. This prevents battery swelling and ensures the power cell lasts for years instead of months.
4. Barcode Scanning
The core differentiator of a medical PDA is its ability to scan. If a nurse has to reposition a medicine vial three times to get a read, the device has failed.
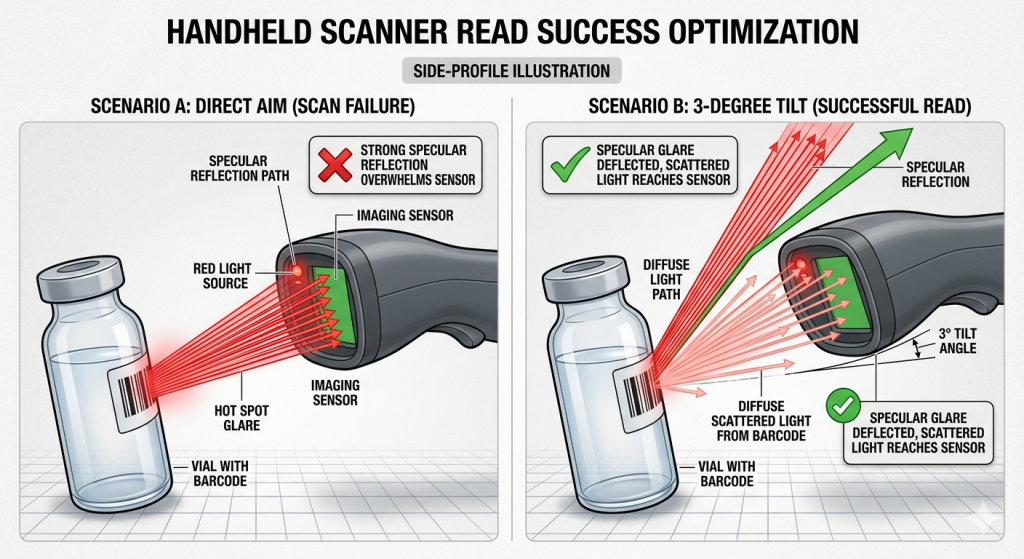
4.1 Solving Specular Reflection
Medicine vials are small, reflective, and curved. They act like moving mirrors. When a scanner’s light hits a vial head-on, the glare (specular reflection) blinds the sensor and collapses the local contrast.
The Engineering Fix:
We did not solve this with a higher-resolution sensor. Instead, we tilted the scanner engine by 3 degrees relative to the housing window. This tiny mechanical cant ensures that the “hot spot” of the reflection bounces away from the sensor. This allows the decoder to see the diffuse light—the light carrying the actual barcode data.
4.2 Accuracy and Reliability Testing
The Standoff Zone
We tuned the decoder exposure for the “standoff zone” (where nurses actually hold the device) rather than ideal flat-label test cards.
Low Light Performance
Optimized sensors for darkened patient rooms where hospital staff must scan without waking the patient.
5. PCB Engineering
Hospital environments are electromagnetically “noisy.” MRI machines and wireless monitors create constant interference. Furthermore, the physical movement of the device introduces mechanical stresses that datasheets often ignore.
5.1 Multi-Layer PCB Design
We utilized an 8-layer HDI (High-Density Interconnect) PCB.
Controlled Impedance
Essential for maintaining Wi-Fi 6 signal integrity.
Isolated Power Domains
The scanner module has an isolated power supply to prevent voltage spikes from affecting the Wi-Fi or CPU domains.

5.2 Connector Failure
A common failure in medical hardware is the board-to-board connector. On paper, they have high mating cycles. In reality, they fail due to micro-fretting.
The Cause
When medical carts roll over elevator gaps or metal thresholds, the vibration causes tiny movements in the connectors. Over time, this creates contact films and intermittent charging or data dropouts.
The Solution
We moved to pogo-pin geometries with floating mechanical compliance. This allows the device to absorb vibration without putting stress on the solder joints.
6. Mechanical Design
At 3:00 AM, medical staff do not follow a manual. They use the fastest shortcut. This is “survival use,” and the mechanical design must reflect it.
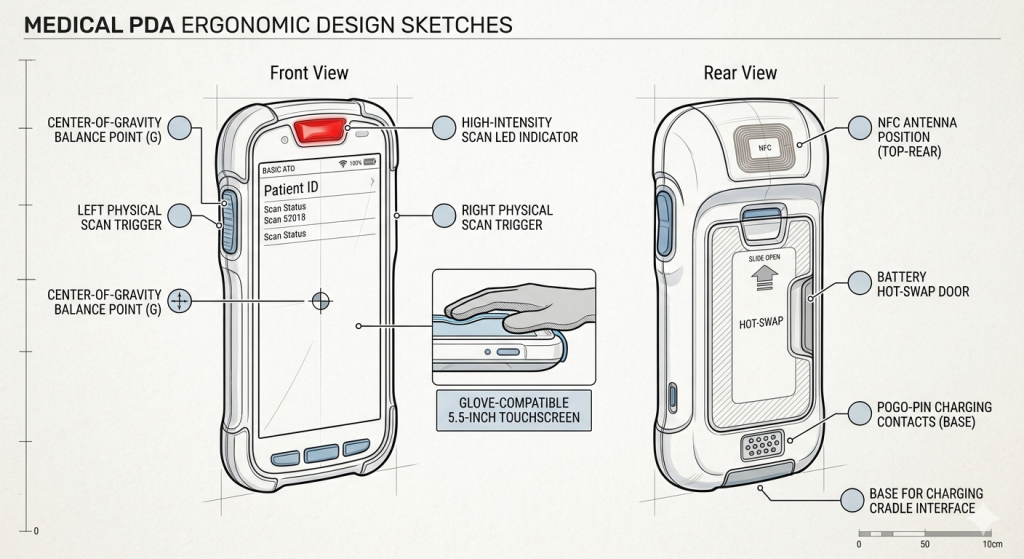
6.1 Ergonomics and Human Haste
- One-Hand Balance: The device is center-balanced so it doesn’t tip when held loosely.
- Parallel Workflow: Nurses often hold meds in one hand and the device in the other. We placed physical scan triggers on both sides for ambidextrous use.
- Feedback Loops: In a noisy ward, a beep is not enough. We implemented high-intensity LED flashes and distinct haptic patterns to confirm a success.
6.2 Disinfection and Wicking Prevention
Standard plastics crack when exposed to hospital-grade disinfectants. We used a medical-grade PC/ABS polymer blend.
Seam Engineering
We eliminated deep seams. When a device is wiped, fluid is pulled into cracks via capillary action (wicking). Our design uses sealed structures to keep chemistry away from internal seals.
Reprocessing Validation
The housing was tested against 5,000 wipe cycles of aggressive chemicals like bleach and Isopropyl Alcohol.
7. Power Management
A “dead” device during a medication pass is a clinical risk. We focused on power reliability through mechanical innovation.
7.1 Long Shift Operation
The PDA uses a 4500mAh high-density battery. We implemented a “hot-swap” feature that allows the battery to be changed without shutting down the OS. This keeps the EMR session active and prevents time-consuming re-logins.
7.2 The Failure of USB Ports
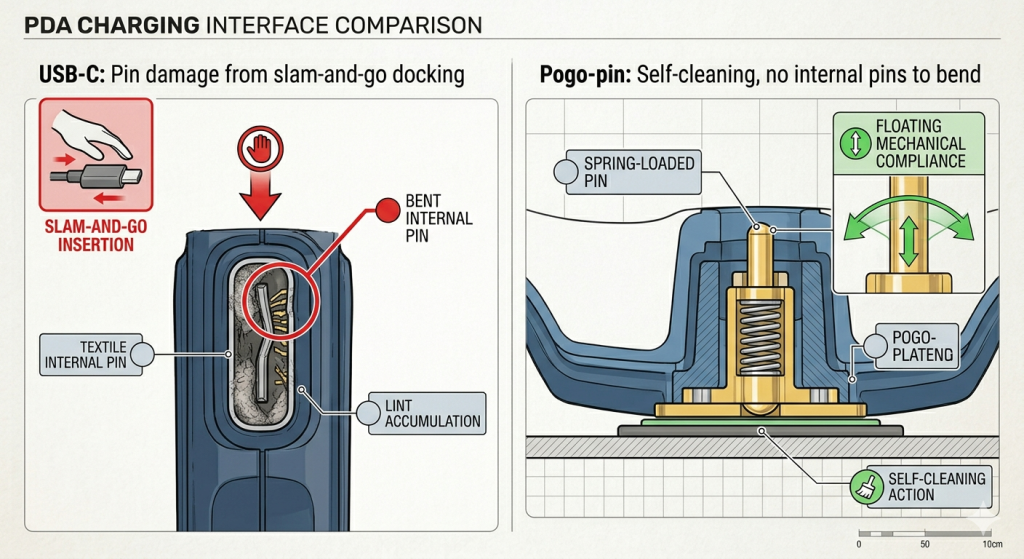
USB-C ports are a failure point in hospitals. They accumulate lint and the internal pins bend under the “slam-and-go” docking style of busy clinicians.
- The Fix: We utilized external pogo-pin contacts for charging. These are self-cleaning and have no internal pins to bend. They provide a much higher mechanical forgiveness during docking events.
8. Android Customization and Hospital Integration
A medical device cannot be a “stock” Android phone. It must be a hardened, single-purpose tool.
8.1 Android Enterprise and Kiosk Mode
We used Kiosk Mode to keep the device limited to clinical apps only. Because of this, users cannot move freely between apps. It stops unnecessary app switching and lowers security risk as well.
Zero-Touch Enrollment
With Android Enterprise, hospital IT teams can set up large numbers of devices in one go. For example, 500 devices can be deployed together with Wi-Fi settings and security certificates already loaded. The staff do not need to open each device one by one. This saves a lot of time and makes rollout easier.
8.2 HIS and EMR Connectivity
We also tuned the Wi-Fi stack for 802.11k, 802.11v, and 802.11r protocols. This is important in a hospital setting. When a nurse moves from one part of the hospital to another, the device can shift to the next access point very quickly, within milliseconds. If this handoff is not smooth, the EMR session may freeze each time the user passes from one ward area to another.
9. Prototyping and Validation: The 5,000-Wipe Test

We moved through three validation phases: EVT (Engineering), DVT (Design), and PVT (Production).
9.1 Reliability Testing
The most brutal test was the Chemical Reprocessing Test. We subjected the device to 5,000 cycles of mechanical wiping using aggressive hospital chemicals.
- Failure Mode Discovery: In early prototypes, we saw “fogging” on the scanner window.
- The Fix: We switched to a chemically hardened glass with a specific anti-reflective coating that did not degrade when exposed to bleach.
9.2 Drop Test
We performed 1.2-meter drop tests on concrete—the typical height of a nurse station. We didn’t just test for a “broken screen.” We tested for “intermittent resets” caused by internal components shifting under impact.
10. Mass Production and Quality Control
Moving from a prototype to 10,000 units requires strict “Medical-Grade” control.
10.1 SMT and PCBA Process
We used X-ray inspection on 100% of the boards to check for solder bridge defects on fine-pitch BGA components. Every board underwent RF calibration to ensure Wi-Fi performance was identical across the entire fleet.
10.2 Traceability and Firmware
Each PDA has its own unique serial number. So it is possible to trace each part easily. We also used a secure firmware flashing process during manufacturing. This was done to make sure no malware could be placed into the device at that stage.
11. Engineering Challenges and Solutions
| Challenge | Risk | Engineering Solution | Result |
| Glare on vials | Scan failure / Manual entry | 3-degree engine cant | 99.9% first-time scan rate |
| Wi-Fi dead zones | Data lag / EMR freezing | Antenna diversity & Wi-Fi 6 | Seamless roaming in wards |
| Chemical cleaning | Case cracking / Seal failure | Medical-grade PC/ABS polymer | Survives 5,000+ wipes |
| Micro-fretting | Intermittent charging | Pogo-pin floating contacts | Long-term mechanical life |
12. Project Outcome and Deployment Results
The final device was successfully integrated into multiple hospital systems, proving that “survival use” engineering pays off.
Clinical Accuracy
Medication errors dropped by 15% due to better scanning on difficult packaging.
Reliability
The hardware failure rate was less than 1% over the first two years of deployment.
Efficiency
Nurses reported saving 20 minutes per shift due to faster “wake-and-scan” response times and reliable Wi-Fi roaming.
Supply Chain
The 7-year chipset guarantee prevented the IT department from having to re-validate their software for new hardware every year.
13. Conclusion
Successful medical handheld development is not about following a checklist of keywords. It is about understanding the “scar tissue” of previous failures. By prioritizing reprocessing validation over IP ratings and optical geometry over sensor resolution, we created a tool that survives the actual clinical environment.
As an expert in Healthcare-grade hardware design and Secure Android customization, we provide end-to-end support from concept to mass production. We don’t just build devices; we build clinical uptime.



